ActivityProfessional.Com Login


renewal cycles. Complete
some now & some later.
and Get 25% off
the Total price!
Buy 3 Courses
and Get 30% off
the Total price!
Buy 4 Courses
and Get 35% off
the Total price!
| Create Account | Login | |


Section 16
Admission and Be Persistant with Change
Table of Contents | NCCAP/NCTRC CE Booklet
a. No magic!
What I do have and I don't have. As stated in the DVD seminar, this Manual and DVD do not contain magic. Volumes one, two, and three in this Series provided you with numerous activities that are what I call object manipulations. In other words, you gave the resident an object like a cap to drop in the bowl as in Volume One; in Volume Two clay to roll; or Same and Different Cards in Volume Three. However, this Course deals with the rather nebulous topic of motivation. So this course is different than the preceding three volumes. Each section of the manual is not filled with items to construct. Each section is filled with ideas regarding how to approach a resident or motivate a resident to become involved. By their very nature these concepts are more vague and less concrete. You will be getting one idea of a Service Project or an assembly line that can be used with a Low Functioning and Alzheimer's resident, as well as an extremely alert resident. So think of this course as providing you with a set of communication tools with a smattering of "object manipulations," like Thera-band stretching. But basically shift your thinking to be receptive to re-evaluating the manner in which you approach your most unmotivated residents. Start to think about: #1. What do I say to get him or her motivated? and #2. What types of choices are staff and I offering these residents?
b. Approach the resident shortly after admission
What is the most important day in the facility in a resident’s life?
The most important day, motivationally, for a resident is the first day he or she is in the facility. On his or her first day in the facility, the resident learns either they do or do not have to go out of their room for meals and activities. Consider setting as a priority resident your next new admission.
So how do you approach your new admission? To streamline the process of figuring out a new admission’s capabilities and limitations in a short amount of time, I have found an Assessment Book to be essential.
c. Assessment Tool #1: Assessment Book
The Assessment Book is simply a set of magazine pictures in two pocket folders. I had one pocket folder for men, and one pocket folder for women.
1. The Men's Folder contained pictures of football, baseball, farming equipment (I’m from Indiana), etc.
2. The Women's Folder had pictures of flowers, cakes, etc. The pictures were large and uncomplicated, without very much detail.
For example, let's say you have a Helen who is a new admission and you are not really sure about her capability.
When approaching her you might…
a. Ask permission: “Helen, I’ve got a picture here. Would you like to look at a picture for me?”
b. Your Helen: “No, I don’t want to see a picture." You could tell right away she has some definite preferences.
c. Open-ended question: Eventually persuade her to look at a picture of a sleeping baby, by saying, “What do you think about that?”
d. Your Helen: “Oh, what a cute baby.”
You gain a lot of information quickly through the use of pictures. With identification of this magazine picture or photo you are able to draw a couple of conclusions from Helen’s statement “Oh, what a cute baby.”
a. Mental and visual assessment: She can identify a picture.
b. Verbal assessment: She can talk.
Word Cards
While putting together your assessment pocket folders, you might also include pictures with words. As you know, Alzheimer’s disease affects the frontal lobes of the brain, which affects recall. However, the ability to read is not controlled by the frontal lobe. This ability is performed in the back of the brain. I have been surprised when residents who speak in gibberish or just make a lot of noises are shown a picture with words printed at the bottom, and they can read the word.
Goal: To read a two or three-word word card…____________________
Eye Assessment & Use of Word Cards
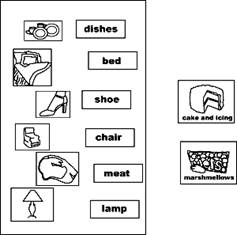
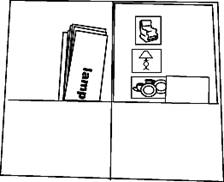 You may say, “So big deal. You walk up, kneel down and show Helen a magazine picture.” Well, if you focus your attention and really look at her eyes, you learn quite a bit about her attention span and alertness level. This will help you to assess the appropriateness of low functioning activity, and write your Care Plan Goal. Remember your Care Plan Conference may be in 20 minutes. All of the above is accomplished in about 1 to 3 minutes. So there you have it, the first step in a quick, easy, but highly effective assessment of your next new admission and starting you on the road to providing them with an activity they will be motivated to become involved with. The illustration above shows a sample of magazine pictures I had pasted to construction paper and added word cards. The second illustration shows magazine pictures on separate cards with the name at the bottom. The third illustration shows a pocket folder with word cards separate from the picture for residents to match the word with the picture.
You may say, “So big deal. You walk up, kneel down and show Helen a magazine picture.” Well, if you focus your attention and really look at her eyes, you learn quite a bit about her attention span and alertness level. This will help you to assess the appropriateness of low functioning activity, and write your Care Plan Goal. Remember your Care Plan Conference may be in 20 minutes. All of the above is accomplished in about 1 to 3 minutes. So there you have it, the first step in a quick, easy, but highly effective assessment of your next new admission and starting you on the road to providing them with an activity they will be motivated to become involved with. The illustration above shows a sample of magazine pictures I had pasted to construction paper and added word cards. The second illustration shows magazine pictures on separate cards with the name at the bottom. The third illustration shows a pocket folder with word cards separate from the picture for residents to match the word with the picture.
Goal: To match two word cards correctly out of four with the corresponding magazine picture…
How to Create Levels of Difficulty
To assemble your Assessment Book, what you might do is have a volunteer or alert resident tear out pictures from magazines. Then cut out any pictures you deem appropriate and make a picture file for yourself. Paste or tape these pictures on corrugated cardboard, poster board, or construction paper. Pictures that you provide a resident for their viewing have different levels of difficulty.
a. A picture of a pastoral or farm scene is sometimes difficult for a resident to identify because it has numerous objects: trees, barns, fences and so on. This idea is expanded upon in Volume 2 when the 3 Piece Puzzle is explained.
b. However, if you take a picture of a pig, for example, and cut out the outline and paste it onto construction paper, then paste that onto your corrugated cardboard, I find it is much easier for a resident to identify an object in isolation. In writing your Goals, you can show a progression by varying the level of difficulty of the picture your Helen is viewing.
Goal: To identify or describe a picture with several objects in it... (That would be the pastoral scene.)
A revised goal simpler than the above, as the resident slips further into Alzheimer’s, would be...
Goal: To identify a picture with one single object in it…
Goal: To identify a picture with one single object in it that has been cut out and mounted on bright paper…
Approach: To cut out the outline of the picture for resident’s easier object identification...
When showing your Helen the picture, assess her eye contact with the picture. Continuously be looking to see where Helen eyes are looking, and whether she is actually focusing on the picture, or whether the residents is just blankly gazing at it or through it, unaware that the object in front of her is different from the wall in the background of her line of vision.
Make a Line of Vision Assessment
Initially, you might position the picture just out of Helen’s line of focus slightly to see if she will move her eyes.
Goal: To have eye contact with picture…
If you move the picture slightly, you might have the following goal.
Goal: To turn head in direction of picture…
Verbal Ability Assessment
If your Helen is able to vocalize, when you show a picture of a sleeping baby, you might ask, “What do you see here?" Thus, asking an open-ended question that cannot be answered by "yes" or "no." If Helen does not respond or gives an inappropriate answer like, “da, da, da,” then start to describe items in the picture. For example, ask "Is this the baby’s head? Is this the baby’s eyes?" If Helen makes a noise or a vocalization, your Care Plan Goal might be as follows.
If she is able to say words, the Care Plan Goal might be…
Goal: To name the baby picture by saying the word “baby”…
Goal: To make the B sound regarding the baby picture…
Approach: To repeat any vocalizations that the resident makes as reinforcement for responding…
For more alert residents, a goal related to picture identification might be as follows:
Goal: To describe the details they see in a picture; naming grass, trees, barn, etc…
Discussion Goals for Severely Contractured Hands
Goals regarding looking at and naming pictures from your Assessment Book or Assessment Folder are oftentimes appropriate goals if Helen has extremely contractured hands. Perhaps your Helen is unable to do object manipulations, like those explained in Volume 1, Shape Sorting; Volume 2, Activity Apron; or Volume 3 Stenciling. Thus, since she cannot hold anything in her hands, she might be able to do Thera Band stretching, to be explained later, or perhaps the Goals above will be the extent of her activity program; i.e. being presented with a magazine picture and naming objects in the picture or having eye contact with the picture.
Approach: To hold magazine picture just out of Helen’s line of vision to encourage her to look and picture, then discuss.
Sometimes residents with short attention spans are agitated and continually walk around the facility. Even though they may have excellent hand coordination, you cannot hold their attention for more than a few seconds. So you might focus your Program and Care Plan Goal on a conversation related to a picture, or maybe just to the here and now. By focusing a conversation on the "here and now," you might state, for example, "I like your dress. Do you like your dress? It’s blue; it’s pretty." Your Goals would focus around a Reality Orientation type of communications. However, by Reality Orientation with an agitated, wandering-level resident, I don’t mean that you would tell the resident that today is Tuesday, it’s two o’clock, and it’s March. Oftentimes, they are too far into their own world for this to be appropriate, as you are well aware.
Care Plan Goals for Wandering, Agitated Residents
Goal: To carry on a two or three word conversation regarding their clothing…
Approach: To start conversation by saying , “I like your dress. Do your like your dress?”
Goal: To give a two to three word response regarding what they are wearing…
Approach: To compliment clothing and comment on color to encourage a focused, appropriate response…
Goal: To name one of the objects in a picture hanging in the facility hall…
Approach: To ask open-ended questions regarding the content of a picture they happen to be standing by, and appear interested in…
Goal: To make a comment about an object outside the window…
Approach: Comment on trees and grass outside the window out of which the resident is staring to encourage conversation…
Residents with whom to use the Assessment Book or Assessment Folder
| Residents | Assess Interest & Ability/Preparation/ Implement |
Staff Member or Volunteer/ When? |
|
|
|
|
|
|
|
|
|
Culture Change CNA Inservice: Brainstorm about residents CNAs feel could benefit from their discussion of photos or magazine pictures.
d. How to Create a "Database" in Your Mind
What do I mean by a Database in your mind, and why do you need one? Let's deal with the "why" first. In order to motivate a resident successfully, I feel I need to know where I am and where I am going regarding the choices I offer a resident. To do this… create an Activity Database in your mind.
1. Have a standardized way of approaching a resident to assess an activity program for him or her.
2. Create a mental picture or a physical list of activities in order form least difficulty to most difficult. You might call this a List or Ladder of Activities in order by Skill-Level.
Why create this mental or written list of activities? When one activity does not work with a resident, you have the mental agility to think of an activity either above it on a subjective Skill-Level Ladder of Activities you have created, or below. In short, is the activity too easy for the resident you have in mind? Would a slightly more difficult activity be appropriate? If so what is a listing of those activities that are more difficult than the one you just tried?
What questions do you use to assess mental capability? Do you know what questions you use? Do you have a standard way of approaching a new admission? By having and being aware of three to four standard questions you ask new admissions, or a resident who has recently gone "down hill," you create a "Database" in your mind for program and Care Plan development. Of course with some residents that are in the end stages of Alzheimer's, you don't get past your introduction. They are clearly not aware of your presence. But, that too goes into your mental data base for program development to motivate your resident.
To create your Database of Activities start with a basic assessment.
#1. "How are you today?" (pause)
#2. "Have you always lived in (name city in which your facility is located)?" (pause)
#3. "What did you used to do?" (pause)
#4. If you have an Assessment Book, show a picture and ask, "What do you see here?"
If you wish to standardize your process of initial assessment, write below questions that are your favorites.
| Assessment Question #1. |
Assessment Question #2. |
Assessment Question #3. |
Assessment Question #4. |
Your Thought Process
When, or if, your Effie does respond to your questions above, the next step is to create a Skill-Level Ladder of Activities in your mind. This Skill-Level Ladder helps you to pair or match your Effie's ability with an appropriate activity she will be motivated to do. Your thought process while asking the above three or four questions might go something like this,
1. Effie can make eye contact and was able to say the word 'fine.'
2. But she shows no response to my other questions.
3. Towel folding would be too hard.
4. However, she might be a good candidate for a simpler activity like dropping a cap into a bowl. Caps-in-a-Bowl is described in Volume 1 of this series.
5. Or, "Effie is fairly clear in her answers. I'll invite her to sing-a-long this afternoon."
What you are doing is arranging a listing of activities in your mind into a Skill-Level Ladder, with the most difficult activity at the top. Then mentally move Effie either up or down, depending upon how she answers your three or four questions and responds to a magazine picture from your Assessment Folder.
Skill-Level Activity Ladder
In summary, if you haven't done so already, develop a three or four question standardized approach for assessing new admissions. Then make a list of Activities from these courses and other Activities. Start with the simplest to most difficult or vise versa. Below is a table to facilitate your thought process when you assess a resident and move them mentally up and/or down the Skill-Level Activity Ladder as you ask your three or four standardized questions. For example if "Clay" does not work perhaps a Pillow Maze will. Or perhaps for a resident with more capability, Lacing Cards are too easy, so you see if the new admission can do yarn weaving.
Thus, as you interview a resident, you are aware of the relative difficulty level of your
Low Functioning and Alzheimer's activities to one another.
Clearly this is not a hard-and-fast relationship between the activities, due to the fact that residents have infinitely varying levels and combinations of mental and physical abilities and limitations. But I suggest you make your own Skill-Level Activity Ladder. Fill in your "favorite" Low Functioning and Alzheimer's activities, as well as other activities. Use it as a general guide to assist this mental assessment process.
The key is to be aware of the activities relationships to one another, concerning their level of difficulty.
Your awareness of the difficulty level of an activity as it relates to another activity facilitates your thought process regarding what to try next when one activity does not work to motivate a resident with a more appropriate activity. Make sense?
Make your Own!
To motivate your unmotivated… take a notebook, word processing program, excel spreadsheet program, etc. and list the current activities that you have for your Low Functioning and Alzheimer's and other residents. Then put these activities in a general order either from most difficult to least or the other way around. Use the table below as a guide to get started. Keep in mind some activities overlap and there are no hard-and-fast rules. This is to serve as a general guide to facilitate your thought process as to what to try next when an activity is either too easy or too difficult for your resident. Clearly you will have a much easier time, motivating your most unmotivated residents, if you are presenting them with activities that match their physical and mental capabilities and limitations, by not being too easy (that they view it as child's play) and not being too difficult (so that they feel like a failure).
Name: |
||||
Activities for Heavy Care Residents |
||||
Warm Damp Cloth – Vol. 3 – AG |
Breathing: Depth and Rate – Vol. 2 – AA |
Activity Apron – Vol. 2 – AA |
||
Cradle Head – Vol. 3 – AG |
Gestures: Hand, Head, & Face – Vol. 2 – AA |
Dolls and Stuffed Animals – Vol. 2 – AA |
||
Room Lighting – Vol. 3 – AG |
Noise, Sound, & Word – Vol. 2 – AA |
Velcro Baseball Mitt – Vol. 2 – AA |
||
Family Photo – Vol. 3 – AG |
Scent Therapy & Smell Can – Vol. 2 – AA |
Balloon Batting – Vol. 2 – AA |
||
Getting in Close – Vol. 3 – AG |
Bouillon Cube Container – Vol. 2 – AA |
Pillow Maze – Vol. 2 – AA |
||
Mobile – Vol. 2 – AA |
Kneeling Pad – Vol. 2 – AA |
Clay – Vol. 2 – AA |
||
Eyes: Openness – Vol. 2 – AA |
Bean Bag Rolling – Vol. 2 – AA |
Communication Board – Vol. 3 – AG |
||
Eye: Movement and Focus – Vol. 2 – AA |
Push Ball – Vol. 3 – AG |
Days Diary – Vol. 3 – AG |
||
Activities for Residents who can/will manipulate an object |
||||
Caps-in-a-Bowl – Vol. 1 – AL |
Bean Scooping – Vol. 2 – AA |
Lacing Cards – Vol. 3 – AG |
||
Bank Exercise – Vol. 1 – AL |
Guess Box – Vol. 4 – AM |
Yarn Weaving – Vol. 3 – AG |
||
Color Sorting – Vol. 1 – AL |
Paper Balling – Vol. 3 – AG |
Grocery Bag Weaving – Vol. 4 – AM |
||
Nuts and Bolts – Vol. 6 – AD |
Clothes Pins – Vol. 2 – AA |
Styrofoam Ball – Vol. 3 – AG |
||
Thera-Band Stretching – Vol. 4 – AM |
Exercise Tape – Vol. 7 - AV |
Adaptive Handle – Vol. 3 – AG |
||
Color Pattern Cards – Vol. 1 – AL |
Yarn Winding on a Tube – Vol. 3 – AG |
Stenciling – Vol. 3 – AG |
||
Geometric Puzzle – Vol. 1 – AL |
Yarn Winding on a Pringles Can – Vol. 3 – AG |
Tracing – Vol. 4 – AM |
||
Shape Sorting Box – Vol. 1 – AL |
Yarn Winding on a Donut – Vol. 3 – AG |
Envelope Stuffing – Vol. 2 – AA |
||
Can Rolling – Vol. 1 – AL |
Magazine Folding – Vol. 3 – AG |
Concentration Game – Vol. 3 – AG |
||
Success Therapy® Bags – Vol. 2 – AA |
Bead Stringing – Vol. 2 – AA |
Same and Different Cards – Vol. 3 – AG |
||
Block Stacking – Vol. 2 – AA |
Three Piece Puzzle – Vol. 3 – AG |
Painting – Vol. 6 – AD |
||
Small Group Activities |
||||
Pet Therapy – Vol. 7 - AV |
Seated Musical Chairs – Vol. 4 – AM |
Travel Club – Vol. 6 – AD |
||
Exercise Wands – Vol. 4 – AM |
Roll Across – Vol. 4 – AM |
Card Holder – Vol. 6 – AD |
||
Fish Game – Vol. 2 – AA |
Shuffle Board – Vol. 4 – AM |
Bingo Adaptations – Vol. 2 – AA |
||
Marshmallow Guessing – Vol. 2 – AA |
Horse Race Game – Vol. 4 – AM |
Help Your Neighbor/Las Vegas – Vol. 4 – AM |
||
Permission is granted to duplicate this page for staff use. Keep in a visible place for easy continual reference.
e. Be Persistent with Change
The "Be persistent with change" point made on the DVD suggests that you are assessing the approaches that Staff and Volunteers are using to motivate residents to become involved. If you or other staff are constantly telling your resident, for example, "You'll have fun", or "We have food at the activity," the resident may not be motivated by either of these. So, as a mini-Inservice, ask your Staff to list three residents who have abilities they are not using. Then, write what each Staff member has said to the resident to try to get him or her involved. The next step is to brainstorm other possible motivational approaches that might be used with that resident. Use this Manual as a springboard for your brain storming. If the resident has family that visits, a Staff member might be appointed to talk to a family member regarding any ideas he or she may have regarding motivational approaches.
Residents to Motivate by using a "Different Approach" than ones used in the past
| Resident | Current Approaches, What is Said… |
List alternative motivational approaches explained on the DVD and in this Manual |
|
"You'll have fun!" |
|
|
|
|
|
|
|
Culture Change CNA Inservice: Brainstorm about residents who CNAs feel could be motivated if the “Approach were Changed.”
NCCAP/NCTRC CE Booklet
Forward to Section 17
Back to Instructor's Guide
Table of Contents
Top